If you’ve started using retinol only to discover your skin suddenly looks worse-with redness, peeling, and breakouts appearing where you once hoped for smooth, youthful skin-you’re experiencing what dermatologists call retinization. And here’s the truth: you’re not alone, and what you’re seeing isn’t necessarily a failure. In fact, temporary worsening is often a sign that retinol is working exactly as intended.
This comprehensive guide, reviewed by dermatological evidence, will walk you through exactly what’s happening beneath your skin’s surface, how to distinguish a normal adjustment from a genuine problem, and the precise steps to minimize irritation while maximizing results. Whether you’re a first-time retinol user or you’ve experienced setbacks, this guide provides the expert knowledge needed to navigate retinol side effects with confidence.
What you’ll learn:
- The complete timeline of retinol side effects and when improvement actually appears
- How to differentiate between normal purging and harmful irritation
- Step-by-step protocols to minimize discomfort for every skin type
- When barrier damage is serious and requires professional intervention
- Exact product strength recommendations for your skin’s starting point
What Is Retinol & Why It Causes Side Effects
Retinol belongs to the retinoid family-a group of vitamin A derivatives that fundamentally alter how your skin cells behave. Understanding the mechanism behind side effects makes it significantly easier to push through the temporary discomfort with confidence rather than anxiety.
The retinoid family hierarchy includes retinol (the gentlest over-the-counter form), retinal/retinaldehyde (approximately 11 times more potent than retinol while maintaining low irritation potential), prescription-strength adapalene, and tretinoin (about 20 times more potent than standard retinol, already in its active retinoic acid form). Each sits at a different point on the strength spectrum, but all work through the same fundamental mechanism: they bind to specific receptors in your skin cells and accelerate cellular turnover.
How retinol actually works is where the magic-and the temporary mess-originates. When retinol penetrates the skin, your cells don’t immediately transform it into retinoic acid (the active form). Instead, they perform a two-step conversion: retinol becomes retinaldehyde, then retinaldehyde becomes retinoic acid. This conversion lag is precisely why retinol is gentler than prescription tretinoin, which is already in its active retinoic acid form and doesn’t require conversion.
Once activated as retinoic acid, it instructs your skin cells to:
- Increase their turnover rate, meaning dead skin cells slough off faster than normal
- Stimulate fibroblasts to produce more collagen
- Reduce sebum production
- Fade hyperpigmentation
- Normalize pore function
Why skin gets worse before better is not a flaw in retinol-it’s the mechanism at work. When your skin suddenly accelerates its natural 28-day cell renewal cycle, you’re essentially forcing years of accumulated debris, impacted sebum, and congestion to the surface faster than your skin can comfortably shed it. Additionally, this accelerated turnover temporarily thins your skin’s outer layer (the stratum corneum), leaving newer, less-protected skin cells exposed. The barrier-your skin’s protective shield of lipids and tight cell junctions-is in a transitional state, neither fully compromised nor fully adapted. This is retinization, and it’s temporary, but it looks uncomfortable in the meantime.
Internal link suggestions: See our complete guide on how retinol works at the cellular level and retinol vs retinoids: the complete strength comparison.
Complete Retinol Side Effects List
Not all side effects are equal. Some indicate your skin is adapting normally; others signal that you need to adjust your approach. This section breaks down the complete spectrum so you can accurately identify what your skin is experiencing.
Normal & Expected Side Effects (Retinization)
What retinization looks like:
Retinization describes the predictable, temporary discomfort your skin experiences as it adapts to accelerated cell turnover. These effects are almost universal and typically indicate that the product is working, not harming your skin.
- Redness and erythema: Mild to moderate flushing, typically most noticeable on the cheeks, nose, and forehead. This appears within the first 1-2 weeks and usually peaks around weeks 2-3. The redness occurs because increased blood flow accompanies the accelerated cell turnover, and your skin is responding to the temporary barrier compromise.
- Peeling and flaking: Dead skin cells shed more rapidly than your body naturally replaces them. This manifests as visible flakes, particularly around the nose, mouth, and chin. Peeling is not a sign of damage-it’s evidence of exfoliation happening at the cellular level. You’ll notice this most prominently in the first 2-4 weeks.
- Dryness and tightness: Your skin feels parched despite moisturizing, and the sensation of tightness becomes noticeable, especially after cleansing or when making facial expressions. This occurs because your barrier is in transition, and the outer layer temporarily has reduced lipid content.
- Mild sensitivity: Products that previously felt gentle now sting slightly. Warm water feels hot. Your skin becomes reactive to temperature changes and minor irritants. This hyperreactivity is temporary and reflects the thinned outer layer of skin currently at the surface.
Timeline for normal retinization:
- Weeks 1-2: Symptoms begin, often subtle (very minor dryness, possibly no visible change yet)
- Weeks 2-4: Peak discomfort-redness, flaking, and sensitivity reach their maximum
- Weeks 4-6: Symptoms begin improving; skin texture noticeably smoother
- Weeks 6-8: Significant improvement; most users report reduced irritation
- By week 12: Most retinization has resolved for properly-dosed users
Research shows that 84% of users experience improved skin texture by week 4, even during the discomfort phase. This texture improvement-smoother feel and more even tone-often appears before visual improvement in lines or discoloration, providing an encouraging sign that the process is working.
Moderate Side Effects (Overuse Signs)
Moderate side effects indicate you’re using retinol at too high a concentration, too frequently, or without adequate barrier support. These are addressable with protocol adjustments-you don’t necessarily need to stop retinol entirely.
- Burning sensation: Distinct stinging or burning that appears immediately after application or within minutes. Unlike mild stinging that occurs with barrier compromise, true burning feels acute and uncomfortable. This often indicates concentration or frequency is too high for your current skin state.
- Pronounced tightness: Your skin feels so tight it’s uncomfortable to move your face. This goes beyond the normal mild tightness of retinization and suggests significant dehydration of the outer layers.
- Visible texture changes: Rough, sandpaper-like patches appear, or your skin develops an uneven, bumpy texture. While retinization causes flaking, this moderate effect involves actual texture changes that persist.
- Excessive dryness despite moisturizing: Your skin remains severely dry even with hydrating products layered generously. This suggests your barrier is genuinely compromised and your skin has lost its ability to hold moisture effectively.
What to do immediately:
- Reduce frequency by half (if using 3x weekly, drop to 1.5x weekly or alternate nights)
- Switch to the buffering method: apply moisturizer first, then retinol, then moisturizer again
- Add a hydrating layer-hyaluronic acid serum or ceramide-rich moisturizer-before retinol
- Increase moisturizer application to 2-3 times daily
- Check that you’re not combining retinol with other exfoliating actives (AHAs, BHAs, vitamin C)
- Most moderate symptoms improve within 1-2 weeks of frequency reduction
Severe Side Effects (Stop Immediately & Contact Dermatologist)
Severe side effects represent genuine barrier damage or allergic reactions that require professional evaluation. Do not continue retinol use if experiencing these symptoms.
- Swelling (edema): Puffy, swollen areas, particularly around the eyes, lips, or across the face. This may indicate allergic reaction or severe barrier damage.
- Hives or urticaria: Raised, itchy welts or a rash that spreads across treated areas. This is typically an allergic response, not simple irritation.
- Barrier damage signs: Raw, open patches; oozing or weeping skin; intense pain from nearly all products; constant feeling that your skin is compromised; peeling so severe it affects daily activities.
- Extreme cases: Nosebleeds or cracking at the corners of the mouth (reported in extreme overuse scenarios with high-strength formulas).
- Persistent symptoms beyond week 8: If after 8 weeks of proper use you’re still experiencing significant redness, burning, or irritation, the product or concentration may not be suitable for your skin.
Immediate action required:
- Discontinue retinol immediately
- Rinse face with cool water only (avoid cleansers temporarily)
- Apply only gentle moisturizer and petroleum jelly as occlusive barrier repair
- Schedule dermatology appointment within 3-5 days
- Do not attempt self-treatment; professional guidance is necessary
Purging vs Bad Reaction: The Critical Distinction
This is the question that keeps most new retinol users awake at night: Am I purging (and should I power through), or am I having a bad reaction (and should I stop)? Getting this distinction right determines whether you continue toward beautiful skin or waste months fighting a losing battle.
| Characteristic | Purging | Irritation | Allergic Reaction |
|---|---|---|---|
| Primary locations | Areas where you already break out (problem zones) | All over treated area, including areas without prior breakouts | Variable, often spreading or concentrated on lips/eyes |
| Type of bump/lesion | Small whiteheads, pustules, sometimes blackheads | General redness, raw patches, texture changes | Hives, welts, swelling, sometimes blistering |
| Appearance | Looks like regular acne breakouts | Diffuse redness, shiny/tight appearance, visible peeling | Raised bumps, localized or spreading inflammation |
| Timing | Begins week 1-2, peaks week 3-4, resolves by week 6-8 | Can start any time, worsens with continued use | Typically within hours to 48 hours of first exposure |
| Associated itch | Minimal; occasional slight itch | Minimal to moderate itch depending on severity | Intense, persistent itching |
| Response to moisturizing | Continues despite hydration; breakouts eventually resolve | Temporarily improves with occlusive products but doesn’t fundamentally improve | Does not improve; may worsen with rich products |
| What to do | Continue retinol at same frequency; add hydrating layers; be patient | Reduce frequency by 50%, add buffering, increase moisturizer; reevaluate in 2 weeks | Stop retinol immediately; see dermatologist; suspect allergen |
Key insight for decision-making: Purging is literally your skin clearing out what it wants to clear out-these breakouts would have appeared eventually, retinol is just accelerating the timeline. They resolve from the inside out as your skin clears. Irritation, by contrast, appears as a consequence of barrier compromise and often worsens if you continue unchanged. Purging improves with hydration and patience; irritation improves with reduced frequency and barrier repair.
Internal link: See our detailed purging vs allergic reaction guide for complex cases.
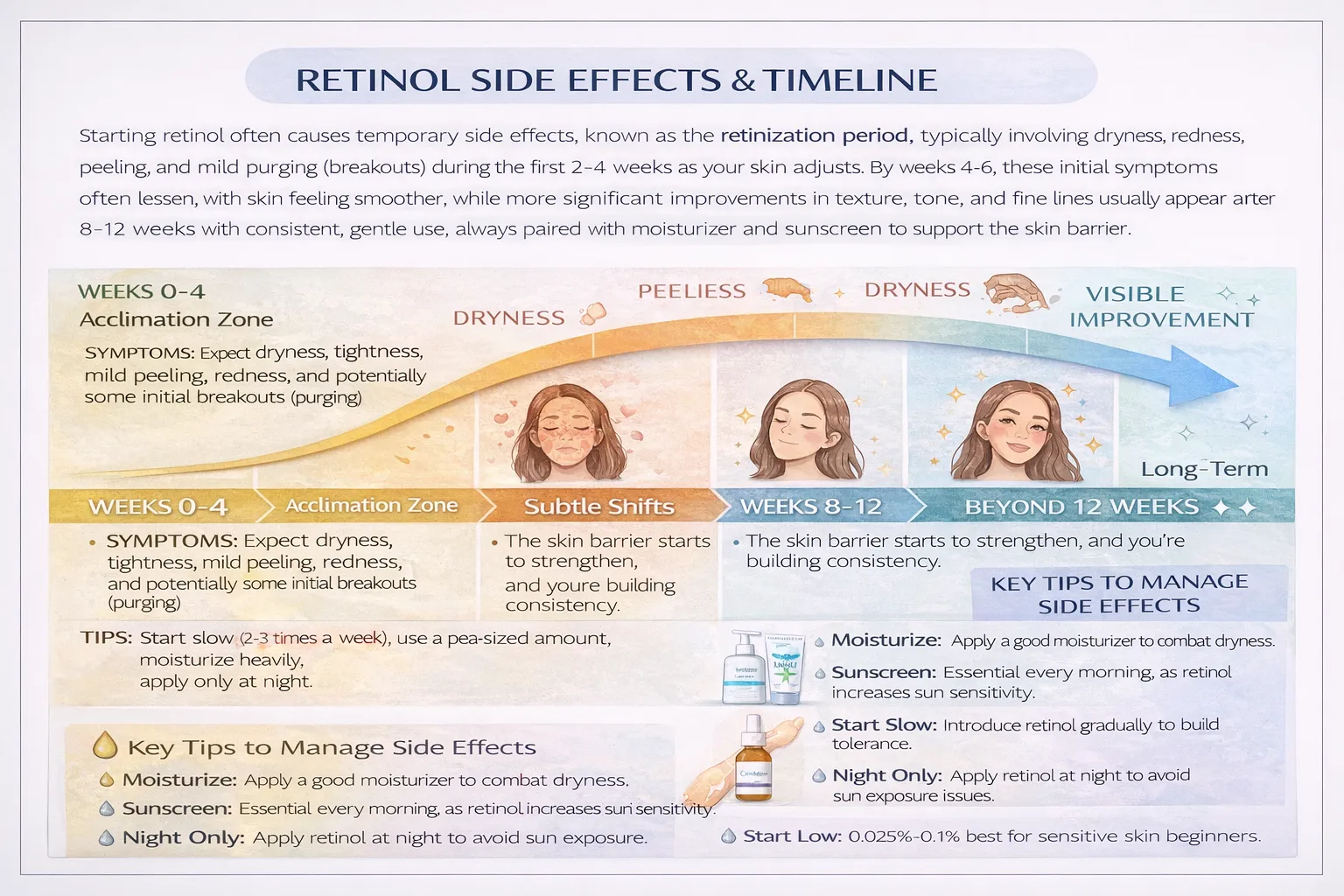
Retinol Side Effects Timeline: Week by Week
This week-by-week breakdown describes the typical progression for someone using 0.25%-0.5% retinol, 2-3 times weekly, with proper moisturizing. Your individual timeline may shift 1-2 weeks based on starting concentration, frequency, and skin sensitivity.
Critical takeaway: If you’re still experiencing significant discomfort at week 8, and it hasn’t notably improved, that’s the signal to investigate whether your concentration, frequency, or supporting routine needs adjustment-or whether consultation with a dermatologist is warranted.
Why Skin Gets Worse Before Better: The Science Behind It
Understanding the mechanism transforms frustration into informed patience. Here’s what’s literally happening beneath the surface.
Accelerated cellular turnover is the foundational mechanism. Your skin naturally renews every 28 days. Retinol compresses this timeline, increasing turnover to roughly every 14-21 days in the early weeks. This isn’t damage-it’s intentional acceleration. However, this speed means your skin is shedding more dead cells than usual while simultaneously not regenerating new cells quite fast enough to keep up. For 3-4 weeks, there’s a slight shortage of fresh, healthy cells at the surface. You’re seeing older, less-protected layers. This is temporary but noticeable.
Debris surfacing describes the process of impacted sebum, bacteria, and congestion rising to the surface. Your pores weren’t necessarily “clogged” in a way you could see, but retinol tells your skin to expel what’s trapped in them. Think of retinol as giving your skin marching orders: “Clear that out.” The sebum that would have gradually released over months now surfaces within weeks. It looks like a breakout, but it’s actually clearing.
Barrier adaptation is the temporary weakening followed by strengthening. Your stratum corneum (the outer layer of skin cells) acts as a protective barrier composed of cells and lipids. Accelerated turnover means these cells are being shed faster than your skin naturally produces replacement lipids. For a few weeks, your barrier is thinner and less protective. Your skin feels dry, sensitive, and reactive. This is not permanent damage-your skin is actively rebuilding this barrier with stronger lipid composition. By week 6-8, your barrier is typically stronger than before you started retinol, with improved water retention and protective function.
Myth-busting:
- Myth: “If retinol causes irritation initially, you should stop.” Truth: Temporary irritation during retinization is expected and does not indicate damage. Severe irritation that doesn’t improve with hydration and reduced frequency warrants adjustment, but mild retinization is a sign the product is working.
- Myth: “Retinol permanently damages your skin barrier.” Truth: When used appropriately, retinol strengthens the barrier long-term. Misuse (combining with other actives, too-high concentration, too-frequent application) can damage the barrier temporarily, but this heals within 3-6 weeks with proper repair protocol.
- Myth: “You can’t use retinol if your skin is sensitive.” Truth: Sensitive skin can use retinol; it simply requires lower starting concentrations (0.1%-0.25%), lower frequency (1-2x weekly), and stronger barrier support. Thousands of sensitive-skin users successfully use retinol long-term.
Side Effects by Skin Type
Your skin type significantly influences both the severity and the management strategy for retinol side effects. Here’s what you should expect based on your skin profile.
Oily & Acne-Prone Skin
Oily skin typically experiences milder initial side effects because the sebaceous glands are already producing adequate lipids. However, oily skin often experiences more noticeable purging because there’s more impacted sebum and congestion in pores for retinol to mobilize.
Expected side effects: Purging with more pronounced acne (often concentrated on the chin, jawline, or forehead), mild redness, some peeling (less severe than dry skin experiences).
Timeline: Purging typically lasts 4-6 weeks; oily skin usually transitions more quickly to the “getting better” phase by week 6-8.
Best approach:
- Start with 0.25%-0.5% retinol, 2x weekly
- Use lightweight, non-comedogenic moisturizers (avoid heavy oils)
- Niacinamide pairs excellently with retinol for oily skin (reduces sebum without increasing irritation)
- Consider pairing retinol with a gentle BHA like salicylic acid, but not simultaneously-alternate nights instead
- By week 8, acne-prone skin should show meaningful breakout reduction
Dry & Sensitive Skin
Dry and sensitive skin experiences the most pronounced initial side effects because there’s less natural lipid cushion. However, this skin type also shows the most dramatic improvement once retinization is complete because the barrier-strengthening benefits of retinol are most noticeable.
Expected side effects: More pronounced redness, more visible peeling, significant dryness, higher risk of tightness and sensitivity to other products.
Timeline: Side effects typically last 6-8 weeks; this skin type needs more patience, but the payoff is substantial.
Best approach:
- Start with 0.1%-0.25% retinol, 1-2x weekly
- Use the sandwich method: moisturizer → retinol → moisturizer
- Layer hydrating products: hyaluronic acid serum under moisturizer before retinol
- Add a facial oil as final layer on retinol nights
- Avoid all exfoliating actives (AHAs, BHAs, vitamin C) during the first 8 weeks
- Pause retinol temporarily if burning becomes intense, resume at lower frequency after 3-5 days
- By week 12, most dry-skin users report their skin feels less dry than before starting retinol (the barrier has strengthened significantly)
Combination Skin
Combination skin presents the mixed challenge of managing different zones with different needs. The T-zone may purge heavily while cheeks experience sensitivity and dryness.
Expected side effects: Varied by zone-oilier areas may show more purging and congestion; drier areas more flaking and sensitivity.
Best approach:
- Apply retinol only to areas that need it (typically not the cheeks if that’s your dry zone)
- Start with 0.25% retinol, 2x weekly
- Use richer moisturizer on dry zones; lighter, niacinamide-rich formula on oily zones
- Layer hydration differently: more hyaluronic acid and ceramides on dry zones
- By week 6-8, you should be able to refine your application strategy based on how each zone responds
Mature Skin (Age 50+)
Mature skin comes with naturally compromised barrier function and slower cell turnover, meaning retinol side effects may be more pronounced initially, but the anti-aging benefits are equally pronounced.
Expected side effects: More visible redness, more pronounced dryness, potentially more pronounced sensitivity, but also faster visible improvement in fine lines and firmness.
Timeline: May need 8-10 weeks for full retinization, but anti-aging results are dramatic.
Best approach:
- Start with 0.1%-0.25% retinol, 1x weekly
- Use the sandwich method consistently
- Pair with peptides, hyaluronic acid, and rich ceramide moisturizers
- Consider adding retinol alternatives first (bakuchiol) for 4 weeks to prepare skin, then introduce retinol
- By week 10-12, most mature skin shows visible fine line softening and improved firmness
Internal link: Complete guide to retinol for sensitive skin.
How to Minimize Retinol Side Effects: The Complete Prevention Protocol
This section provides the exact operational steps to use retinol with minimal discomfort while preserving efficacy. These aren’t suggestions-they’re the evidence-based protocols dermatologists recommend to new retinol users.
The Start Low, Go Slow Protocol
This is the foundational approach that prevents 70% of retinol side effect complaints.
Week 1-2: Introduction Phase
- Choose 0.25% retinol (or 0.1% if you have very sensitive skin)
- Apply 1x per week only
- Apply to entirely clean, completely dry skin (moisture increases absorption and irritation)
- Use pea-sized amount for entire face
- Wait 20 minutes after cleansing before application (let skin fully dry)
- Follow immediately with lightweight moisturizer (within 5 minutes)
- Use only on nights you’re not exposing skin to sun the next day
Week 3-4: Gradual Increase
- Increase to 1x every 5-6 days (so roughly 1.5x weekly)
- Same application protocol as phase 1
- If no significant irritation, proceed to next phase
Week 5-6: Building Tolerance
- Increase to 2x weekly (e.g., Monday and Thursday nights)
- Same application protocol
- If skin is tolerating well and showing adaptation signs, proceed to next phase
Week 7-8: Approaching Regular Use
- Increase to 2-3x weekly based on comfort
- Most people find 3x weekly as their ideal maintenance frequency
- By this point, retinization should be substantially improved
Week 9+: Maintenance
- Use 3x weekly indefinitely for anti-aging benefits
- Nightly use is possible for experienced users whose skin is fully adapted, but 3x weekly provides 90% of the benefits with less irritation risk
The Buffering Method (For Sensitive Skin)
Buffering is applying a layer of moisturizer before retinol to reduce irritation while maintaining efficacy. This is not a permanent workaround-it’s a tool for the sensitive skin during the first 6-8 weeks.
- Cleanse and completely dry skin
- Apply lightweight hydrating moisturizer (wait 3-5 minutes for it to set)
- Apply pea-sized amount of retinol over moisturizer (this is “buffered” retinol)
- Wait 5 minutes
- Apply second layer of richer moisturizer
- Optional: apply facial oil on top for extra occlusion
Buffering reduces irritation by 40-50% while maintaining roughly 80% of retinol efficacy. It’s particularly valuable for weeks 3-6 when retinization is most pronounced.
Compatible Routine Architecture
What you use alongside retinol matters significantly.
On retinol nights (2-3x weekly):
- Gentle, sulfate-free cleanser (oil cleanser or micellar water ideal)
- Hydrating toner or essence
- Retinol
- Moisturizer
- Optional: facial oil or occlusive balm as final layer
- SPF 50+ sunscreen the next morning (non-negotiable)
On non-retinol nights (4-5x weekly):
- Gentle cleanser
- Hydrating toner or essence
- Gentle active if desired (but recommended to avoid other actives in the first 8 weeks)
- Moisturizer
- Optional: facial oil
Critical pairing principle: Retinol nights should be “minimalist nights”-you’re using retinol as the active, so everything else should be supporting and soothing, not active.
What NOT to Combine with Retinol
These combinations cause severe irritation and barrier damage when used simultaneously. You can use these ingredients, just not on the same nights as retinol.
Absolute no-combinations:
- Retinol + AHAs (glycolic, lactic acid): Combined exfoliating effect overwhelms barrier; can cause significant damage
- Retinol + BHAs (salicylic acid): Same issue as AHAs; excessive exfoliation
- Retinol + High-strength Vitamin C (L-ascorbic acid): Reduces effectiveness of both; causes irritation
Use on alternate nights instead:
- Retinol on Monday, Thursday, Saturday
- Vitamin C on Tuesday, Friday (separate from retinol by at least 24 hours)
- AHA/BHA on Wednesday only, if at all during the first 8 weeks (generally avoid during retinization)
Safe to use with retinol (same nights):
- Niacinamide: Reduces sebum production without irritation
- Hyaluronic acid: Increases hydration
- Ceramides: Strengthen barrier
- Glycerin: Humectant, adds hydration
- Centella asiatica: Soothes and anti-inflammatory
- Azelaic acid: Actually pairs well; consider for acne-prone skin
- Peptides: Support barrier and collagen
Exact Application Rules
Frequency mistakes account for 60% of retinol complaints:
- Starting too frequently (daily is too much initially)
- Increasing frequency too fast (jump from 1x weekly to 3x weekly in week 2)
- Not respecting the skin’s adaptation timeline
Amount mistakes account for 25% of complaints:
- Using too much product (pea-sized is the maximum; most people can start with a grain of rice size)
- Applying to damp skin (increases penetration and irritation)
- Reapplying if you forgot to use it a night (don’t double-apply)
Timing mistakes account for 15% of complaints:
- Applying directly after cleansing while skin is still damp
- Not waiting 20 minutes after cleansing before application
- Applying sunscreen immediately after retinol (the previous evening’s application is sufficient)
Correct application sequence:
- Cleanse thoroughly
- Wait 20 minutes for skin to completely dry
- Wait 3-5 minutes after applying toner/hydrating layer to fully absorb
- Apply pea-sized retinol, spreading gently across face (avoiding immediate eye area initially)
- Wait 5 minutes before applying moisturizer
- Moisturize generously
- Optional: add facial oil as final layer
- Use SPF 50+ the next morning
Who Should NOT Use Retinol
Retinol is appropriate for most skin types, but several populations should avoid it entirely or use it only under dermatological supervision.
Pregnancy & Breastfeeding
Status: Avoid completely
While topical retinol absorption is relatively low (1-2% systemic absorption from skin application), the potential risks during pregnancy outweigh any skincare benefits. Retinol is fat-soluble and can accumulate in body tissues over time. Oral retinoids (like isotretinoin for severe acne) carry a 20-30% birth defect risk when used during pregnancy, including craniofacial malformations, cardiac abnormalities, and CNS issues.
Recommendation: Stop topical retinol at least 1 month before conception if actively trying to conceive. During pregnancy and breastfeeding, choose alternatives like glycolic acid (gentle concentration), azelaic acid, or niacinamide.
Active Infections or Inflammatory Skin Conditions
Status: Avoid temporarily
If you currently have active bacterial acne, fungal infection, or viral conditions (like cold sores), retinol can worsen inflammation temporarily. Additionally, conditions like rosacea, severe eczema, or psoriasis in flare phases typically don’t tolerate retinol well initially.
Recommendation: Treat the acute condition first, then introduce retinol at lower concentration once stable. For chronic conditions like rosacea, use very low concentration (0.1%) and consult dermatologist first.
Recent Procedures or Chemical Peels
Status: Avoid for 7-14 days post-procedure
If you’ve recently had laser treatment, chemical peels, microdermabrasion, or dermaplane, your barrier is compromised and retinol will cause excessive irritation.
Recommendation: Wait at least 1-2 weeks (or until redness from procedure fully resolves) before resuming retinol.
Extreme Sensitivity or Compromised Barrier Damage
Status: Repair barrier first, then introduce cautiously
If your skin barrier is severely damaged (characterized by burning from nearly all products, intense inflammation, visible damage), starting retinol will worsen the condition.
Recommendation: Spend 4-6 weeks on barrier repair protocol (ceramides, niacinamide, hyaluronic acid, gentle moisturizer, sunscreen), then introduce retinol at minimal concentration (0.05% if possible).
OTC Retinol vs Prescription Retinoids: Complete Comparison
Understanding where retinol sits in the retinoid family helps you choose the right starting point and set realistic expectations.
| Product | Potency | Prescription Status | Irritation Potential | Timeline to Results | Best For | Starting Concentration |
|---|---|---|---|---|---|---|
| Retinol | Weakest OTC | Over-the-counter | Low to moderate | 8-12 weeks for visible results | Beginners, sensitive skin, preventative anti-aging | 0.1%-0.3% |
| Retinal (Retinaldehyde) | 11x stronger than retinol | Over-the-counter | Low (surprisingly) | 4-6 weeks for visible results | Blemish-prone, mature skin, sensitive skin (upgraded strength) | 0.1%-0.5% |
| Adapalene | Prescription-strength | Prescription (though OTC availability expanding) | Moderate | 6-8 weeks | Acne treatment, more resilient skin | 0.1% |
| Tretinoin (Retinoic Acid) | 20x stronger than retinol | Prescription only | Moderate to high | 3-4 weeks | Severe acne, pronounced photodamage, significant wrinkles | 0.025%-0.05% initially |
| Tazarotene | Extremely potent | Prescription only | High | 3-4 weeks | Severe acne, extreme photodamage (requires close monitoring) | 0.025% only |
Key distinctions:
Retinol vs Retinal: Retinal is the direct precursor to retinoic acid (it requires only one conversion step, whereas retinol requires two). This means retinal is roughly 11 times more potent while maintaining similarly low irritation. If retinol results are too subtle, retinal is the logical next step before jumping to prescription options.
Retinol vs Tretinoin: Tretinoin is already in its active retinoic acid form, so there’s no conversion step. It works immediately and intensely, delivering faster results but with higher irritation potential. Tretinoin is typically prescribed for severe acne or dermatological conditions rather than general anti-aging, though it’s increasingly used off-label for aggressive anti-aging goals.
Recommendation hierarchy by need:
- For anti-aging on normal skin: Start with 0.3% retinol
- For acne on sensitive skin: Start with 0.1% retinal
- For significant acne: Retinal 0.3-0.5% or consult dermatologist for adapalene/tretinoin
- For aggressive anti-aging after retinol experience: Consider prescription retinal or tretinoin under dermatological supervision
- For severe acne: Typically tretinoin or tazarotene under dermatological supervision
Internal link: Detailed retinol vs tretinoin comparison.
Retinol Burn: Emergency Recovery Protocol
“Retinol burn” describes the state of severe barrier damage and irritation from retinol overuse. If you’re experiencing this, here’s exactly how to recover.
Symptoms of Retinol Burn
- Intense burning or stinging from nearly all products
- Widespread redness and inflammation
- Raw or weeping patches
- Severe flaking or peeling
- Extreme dryness unresponsive to moisturizing
- Swelling or puffiness
- Hypersensitivity to temperature and touch
- Pain or discomfort throughout the day
7-Day Emergency Stabilization Protocol
Days 1-3: Complete Pause
- Stop all active ingredients immediately (retinol, vitamin C, AHAs, BHAs, all actives)
- Cleanse with water only or gentle micellar water (no sulfates)
- Apply only: gentle moisturizer + petroleum jelly as occlusive layer
- Apply this routine 2-3x daily
- Do not apply makeup
- Avoid sun exposure; if necessary, use mineral sunscreen only (chemical sunscreens may irritate)
- Goal: Stop additional damage and allow acute inflammation to begin settling
Days 4-7: Gentle Repair
- Continue water-only cleansing
- Introduce barrier-repair ingredients: ceramides, hyaluronic acid, niacinamide (5%)
- Simple routine: cleanser → hydrating toner → barrier repair serum → rich moisturizer → petroleum jelly
- Apply 2x daily
- Continue avoiding all actives
- Mineral sunscreen only
- Goal: Rebuild barrier structure
2-4 Week Active Repair Phase
Once acute symptoms settle (usually by day 7-10):
- Continue barrier-repair routine
- Introduce gentle products one at a time, waiting 2-3 days between additions
- Consider adding antioxidant serum (green tea, resveratrol) for anti-inflammatory benefits
- Still avoid all actives
- Use only gentle cleansing
- By week 3-4, most barrier damage shows significant improvement
Reintroducing Retinol After Burn
Weeks 5-6:
- Once barrier feels normal (no stinging from moisturizer, reduced sensitivity), you can consider reintroduction
- Wait a full 5-6 weeks before retrying
- Start with extremely low concentration (0.05% if possible)
- Start with 1x every 10 days (once every 10 days, not weekly)
- Use buffering method: moisturizer → retinol → moisturizer
- If any stinging occurs, return to pause phase for another 3-5 days
- Increase frequency very slowly (every 2 weeks, increase by 1 additional application per month)
Most people fully recover from retinol burn within 4-6 weeks with consistent barrier repair. However, don’t rush reintroduction-a slower, gentler reintroduction prevents recurrence.
Internal link: Complete barrier repair guide.
Product Strength Guide: Choosing Your Starting Point
| Experience Level | Recommended Concentration | Recommended Formulation | Starting Frequency | Best For |
|---|---|---|---|---|
| Beginner with sensitive skin | 0.1%-0.15% | Encapsulated retinol or retinol ester | 1x weekly | First-time users; reactive skin; building tolerance |
| Beginner with normal skin | 0.25%-0.3% | Any form (encapsulated or traditional) | 1-2x weekly | First-time users; non-sensitive skin |
| Beginner with oily/acne-prone skin | 0.25%-0.5% | Can be higher concentration; encapsulation not necessary | 2-3x weekly | Acne treatment + anti-aging |
| Intermediate (3+ months consistent use) | 0.5%-0.75% | Any form; can experiment with pure retinol | 3x weekly or nightly | Wanting stronger results; skin fully adapted |
| Advanced (6+ months consistent use) | 1% | Pure retinol or upgraded to retinal 0.5%+ | Nightly if desired | Maximum anti-aging benefits; full tolerance |
| Prescription options | Adapalene, tretinoin | Prescription strength | Per dermatologist | Significant acne, photodamage, or dermatological recommendation |
Formulation types to know:
- Encapsulated retinol: Retinol wrapped in liposomes or other carriers; releases slowly; less irritation than free retinol; ideal for sensitive skin
- Retinol esters (retinyl palmitate, retinyl acetate): Gentler than free retinol; require additional conversion steps; slower results
- Pure retinol: Direct retinol without encapsulation; fastest results; highest irritation potential
- Retinal (retinaldehyde): Pre-converted form; more potent than retinol; surprisingly low irritation despite strength
Internal link: Best retinol products for beginners.
When to See a Dermatologist
Knowing when professional guidance is necessary prevents unnecessary suffering and ensures you’re not misinterpreting concerning symptoms as normal retinization.
Symptoms Requiring Dermatological Evaluation
Urgent (within 3-5 days):
- Swelling or hives
- Difficulty breathing or throat tightness (potential allergic reaction-seek emergency care if severe)
- Raw, open patches of skin
- Signs of infection (pus, warmth, odor)
Within 1-2 weeks:
- Irritation persisting beyond 8 weeks despite proper use protocol
- Inability to distinguish between purging and problematic reaction
- Recurrent perioral dermatitis or localized severe reactions
- Questioning whether specific skin condition is contraindicated for retinol
Within 3-4 weeks:
- Considering prescription retinoids and wanting professional guidance
- Severe photodamage or acne wanting aggressive treatment beyond OTC retinol
- History of very sensitive skin or compromised barrier; wanting expert protocol
What Dermatologists Will Evaluate
- Current skin condition: Barrier health, existing conditions, sensitivities
- Retinol application protocol: Frequency, concentration, application method-often the issue is technique, not the product
- Skincare routine compatibility: What you’re combining retinol with (frequently, the issue is combining incompatible products)
- Concentration appropriateness: Whether your current strength matches your skin’s tolerance
- Alternative options: If retinol isn’t working, they can recommend retinal, prescription options, or entirely different approaches
Frequently Asked Questions (FAQ Section – Schema Ready)
Q1: How long do retinol side effects last?
Most retinol side effects resolve within 4-8 weeks with proper use protocol. Redness and peeling typically peak in weeks 2-3 and substantially improve by week 6. If symptoms persist beyond 8 weeks without improvement, reduce frequency or concentration.
Q2: Is retinol purging normal and should I power through?
Yes, mild purging is normal and indicates skin clearing congestion. Purging appears in areas where you already break out and resolves in 4-6 weeks. If irritation is severe, burning, or spreading to new areas, reduce frequency rather than continuing unchanged.
Q3: Can I use retinol in summer?
Yes, but with strict SPF 50+ daily application. Retinol doesn’t inherently cause sun damage, but retinized skin (skin with accelerated turnover) is more vulnerable to UV damage. Many dermatologists recommend starting retinol in fall/winter for easier sun protection, then maintaining year-round with proper sunscreen.
Q4: Can I mix retinol with other active ingredients?
Avoid combining retinol with AHAs, BHAs, or high-strength vitamin C on the same nights. Use these on alternate nights, separated by at least 24 hours. Niacinamide, hyaluronic acid, and ceramides are safe to use with retinol.
Q5: Can retinol permanently damage my skin?
No. When used properly, retinol strengthens skin long-term. Misuse (extreme overuse, combining with incompatible actives, ignoring barrier compromise signs) can cause temporary barrier damage, but this heals completely within 3-6 weeks with proper care.
Q6: Why are my lips swollen after using retinol?
Lips are highly sensitive and absorb retinol more readily. If lips swell after retinol application, you may be applying too close to lips or the concentration is too high for your tolerance. Use lip balm as a barrier, avoid lip area application initially, and consider buffering method.
Q7: Can retinol cause headaches?
Retinol should not cause headaches directly. If experiencing headaches, consider: dehydration (retinol can increase water loss-drink more water), sensitivity reaction (see dermatologist), or unrelated cause. Headaches are not a typical retinol side effect.
Q8: Is long-term retinol use safe?
Yes. Clinical evidence shows retinol safety and continued benefits with use up to 24 months and beyond. Retinol strengthens skin barrier with long-term use and continues improving collagen production. Most dermatologists recommend long-term, consistent retinol use for anti-aging.
Q9: Can I use retinol if I have rosacea?
Potentially, but with extreme caution and dermatological guidance. Start with 0.05% retinol, 1x weekly, with heavy buffering and barrier support. Some rosacea improves with retinol’s collagen-building benefits; others are triggered by retinol. Professional guidance is recommended.
Q10: What’s the difference between retinol and prescription tretinoin?
Tretinoin is 20 times more potent than retinol, already in active retinoic acid form, and prescription-only. Retinol is gentler, OTC, requires conversion in skin, and has slower onset. Tretinoin delivers faster results but with higher irritation potential. Choose based on your skin’s tolerance and treatment goals.
Final Takeaways: Your Retinol Success Roadmap
Retinol side effects are not obstacles-they’re evidence that a powerful ingredient is working to transform your skin. Armed with understanding of what’s happening, why it’s happening, and exactly how to support your skin through the process, you can confidently navigate retinization and reach the long-term benefits that make retinol one of dermatology’s most validated anti-aging ingredients.
Your essential action steps:
- Choose your starting concentration based on skin type: 0.1%-0.15% for sensitive skin, 0.25%-0.3% for normal skin, 0.25%-0.5% for oily skin.
- Start with 1x weekly, increasing frequency by one additional application every 2-3 weeks, reaching 3x weekly by week 8.
- Use the sandwich method if experiencing irritation: moisturizer → retinol → moisturizer.
- Avoid incompatible actives (AHAs, BHAs, high-strength vitamin C) on retinol nights for the first 8 weeks.
- Support your barrier with ceramides, hyaluronic acid, niacinamide, and consistent moisturizing.
- Use SPF 50+ daily without exception-retinized skin is more sun-sensitive.
- Expect 8-12 weeks before seeing dramatic results; commit to at least this timeline before evaluating efficacy.
- See a dermatologist if irritation persists beyond 8 weeks, if you experience severe reactions, or if you’re unsure whether you’re purging or having a bad reaction.
Related guides you should explore:
- Best retinol products for beginners
- Retinol alternatives for those who can’t tolerate it
- Before & after retinol timelines
- Retinol for specific skin concerns: acne, wrinkles, hyperpigmentation
- How to build a complete anti-aging routine with retinol
The temporary discomfort of retinization is the price of transformation. Every person currently enjoying smooth, firm, youthful skin powered by retinol once sat where you are-confused by the flaking, frustrated by the redness, questioning whether to continue. They pushed through. You can too. And in 3 months, you’ll understand why retinol remains dermatology’s gold standard for aging skin.
Citations
Medik8. “Tretinoin vs Retinol vs Retinal: What’s The Difference?” Medik8, 2024.
Retinoid potency research from multiple clinical studies cited in research compilation.
Symphonic MD. “Retinol Timeline: How Long Does Retinol Take to Work?” Symphonic MD, 2023.
Stanford Medicine. “Does retinol deserve the hype? A Stanford dermatologist weighs in.” Stanford Medicine, 2020.
Ningen.com. “How Long Does Retinol Take to Work” 2025.
Multiple clinical studies demonstrating 10-12 week improvement in wrinkle appearance.
Face Beauty Science. “Medical-Grade Skincare Results Timeline.” 2025.
Retinoic Acid Embryopathy research from PMC. 2017.
Isotretinoin, Vitamin A Supplements, and Unintended Pregnancies research. 2022.